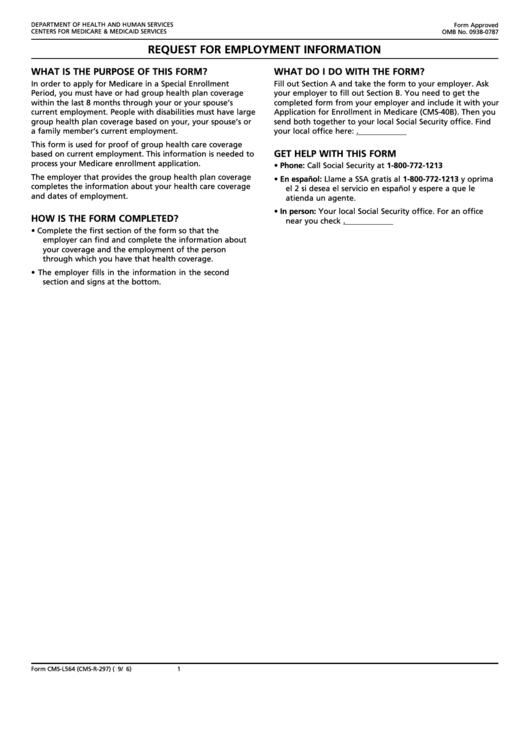
Cms L564 Printable Form - • your employer will need to complete the second half of the form with your employment dates and dates of your group health plan coverage. This information is needed to process your medicare enrollment application. Web cms l564 form printable. Department of health and human services centers for medicare & medicaid services form approved omb no. Web form approved omb no. Concerned parties names, places of residence and phone numbers etc. In order to apply for medicare in a special enrollment period, you must have or had group health plan coverage within the last 8 months through your or your spouse’s current employment. • your basic information and employer name other important information: The person applying for medicare completes all of section a. Write the date that you’re filling out the request for employment.
Form CmsL564 Request For Employment Information printable pdf download
Get help with this form the employer that provides the group health plan coverage completes the information about your health care coverage and dates of employment. Concerned parties names, places of residence and phone numbers etc. Easily fill out pdf blank, edit, and sign them. Web form approved omb no. Giving the social security administration proof you’re eligible to sign.
Form CmsL564 Request For Employment Information, Medicare True/false
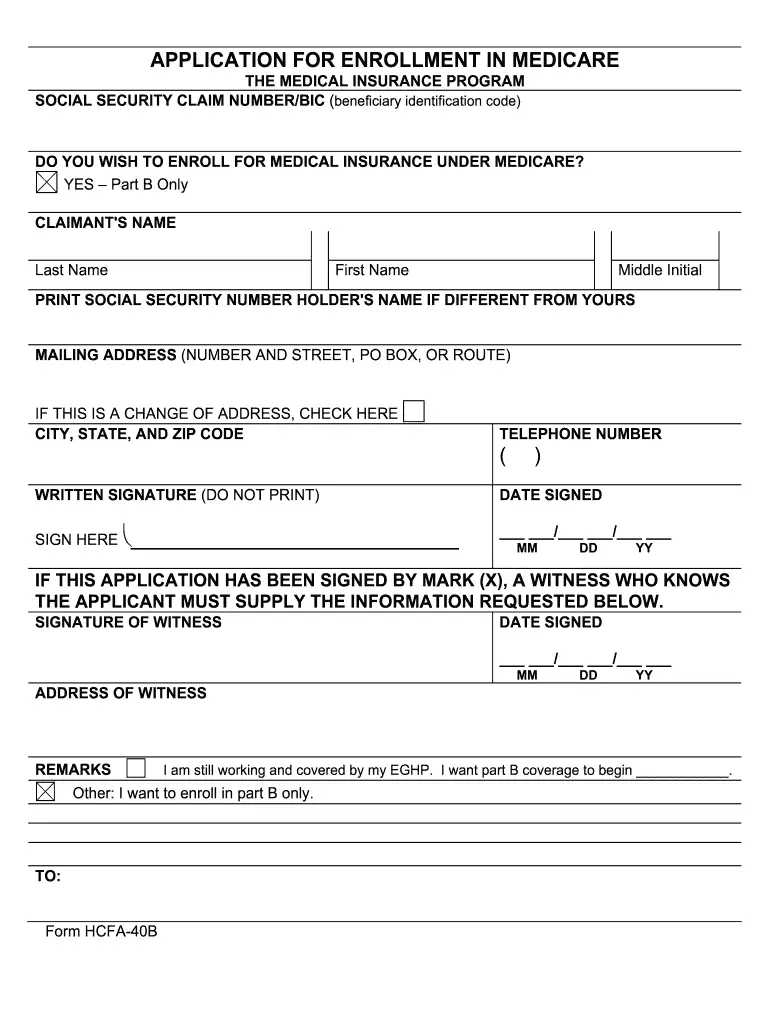
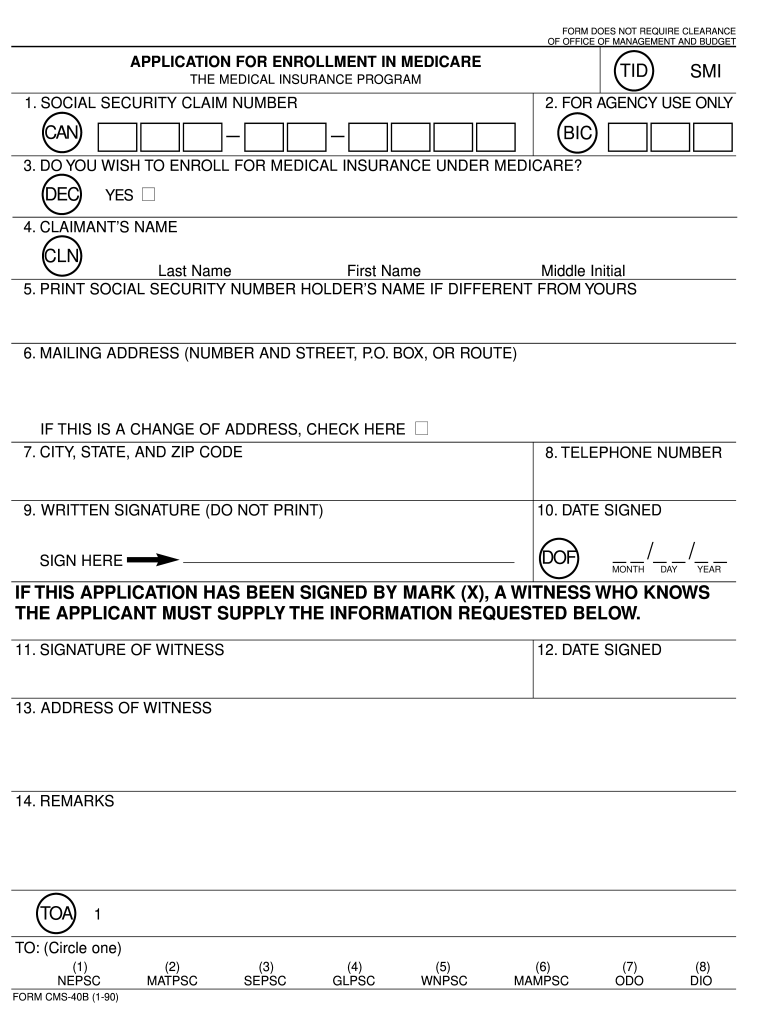
Web form approved omb no. Send your completed and signed application to your local social security office. 06/2023departme nt of health and human services centers for medicare & medicaid servicesrequest for employment information cms 40b form i want part b coverage to begin. Write the name of your employer. Choose the correct version of the editable pdf form from the.

Medicare Part B Application Form Cms L564 Form Resume Examples
Use the redaction tool to black out any sensitive information, such as social security numbers or personal addresses. Choose the correct version of the editable pdf form from the list and get started filling it out. Send your completed and signed application to your local social security office. Change the template with unique fillable areas. Giving the social security administration.
Fillable Form CmsL564 (CmsR297) Request For Employment Information
Choose the correct version of the editable pdf form from the list and get started filling it out. Their spouses can join the plan as well and fill this template out. You may also use the search feature to more quickly locate information for a specific form number or form title. Download your information to pdf before printing. Web find.

Gallery of Social Security Medicare form Cms L564 Awesome 54 Awesome
Web cms forms list. Web cms l564 form printable. Other i want to enroll in part b only. Get help with this form the employer that provides the group health plan coverage completes the information about your health care coverage and dates of employment. Write the date that you’re filling out the request for employment.
How To Fill Out Medicare Part B Application
Easily fill out pdf blank, edit, and sign them. Get help with this form the employer that provides the group health plan coverage completes the information about your health care coverage and dates of employment. The person applying for medicare completes all of section a. According to the paperwork reduction act of 1995, no persons are required to respond to.
20162021 Form CMSL564 Fill Online, Printable, Fillable, Blank pdfFiller
Save or instantly send your ready documents. Get help with this form the employer that provides the group health plan coverage completes the information about your health care coverage and dates of employment. • your basic information and employer name other important information: Get everything done in minutes. Web find and fill out the correct form cms l564 printable.
1990 Form CMS40B Fill Online, Printable, Fillable, Blank pdfFiller
Web related to print form cms l564 cms l564 form approved omb no. 06/2023departme nt of health and human services centers for medicare & medicaid servicesrequest for employment information cms 40b form i want part b coverage to begin. You can also fax your enrollment forms and evidence of employment and health coverage to your local social security office. If.

2005 Form CMS20031 Fill Online, Printable, Fillable, Blank pdfFiller
Download your information to pdf before printing. Use the redaction tool to black out any sensitive information, such as social security numbers or personal addresses. Get everything done in minutes. • your employer will need to complete the second half of the form with your employment dates and dates of your group health plan coverage. Send your completed and signed.
Cms 84 fillable form Fill out & sign online DocHub
You may also use the search feature to more quickly locate information for a specific form number or form title. The information provided in section b is the evidence of ghp or lghp coverage. Web download and print to pdf. What is the purpose of this form? Web cms forms list.
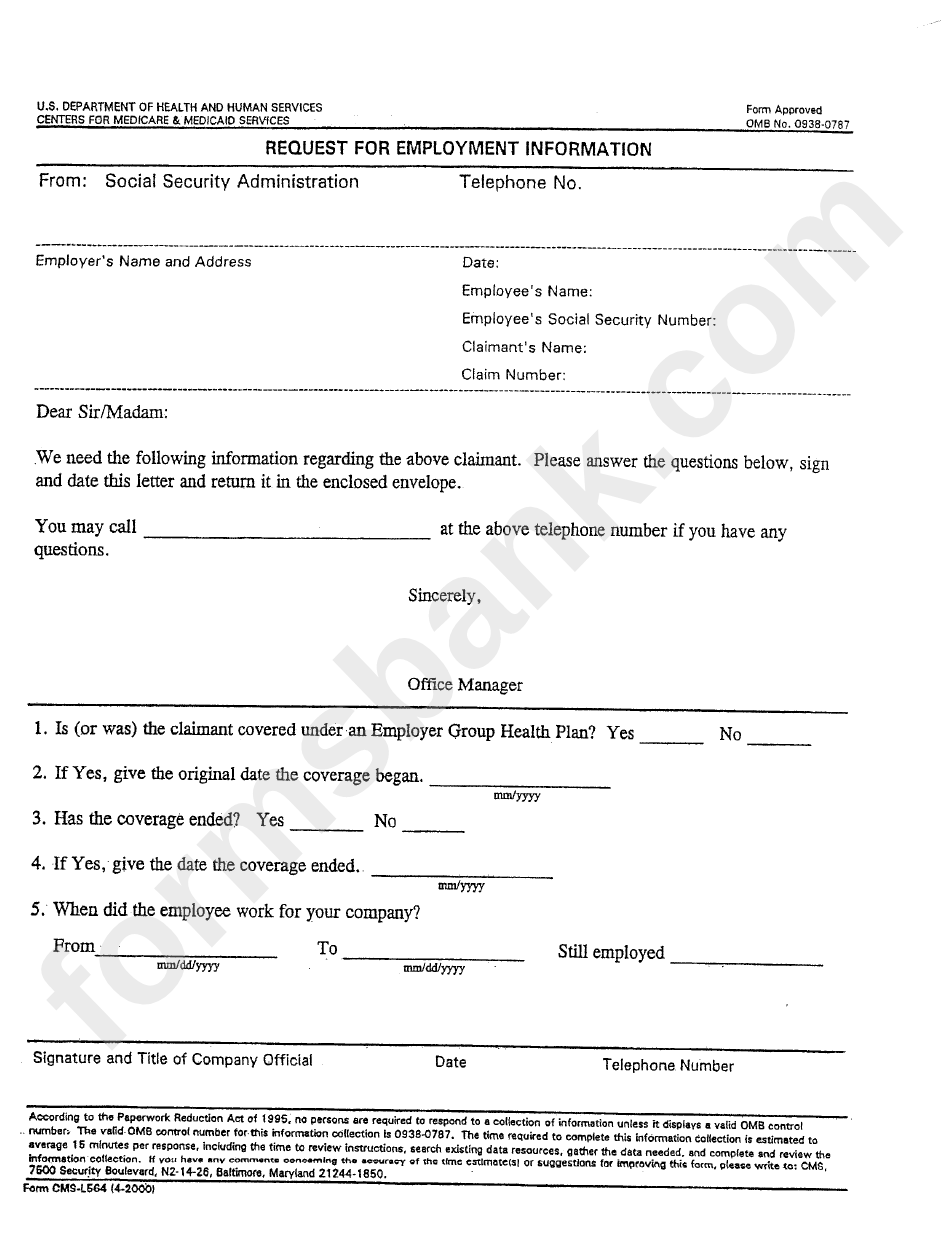
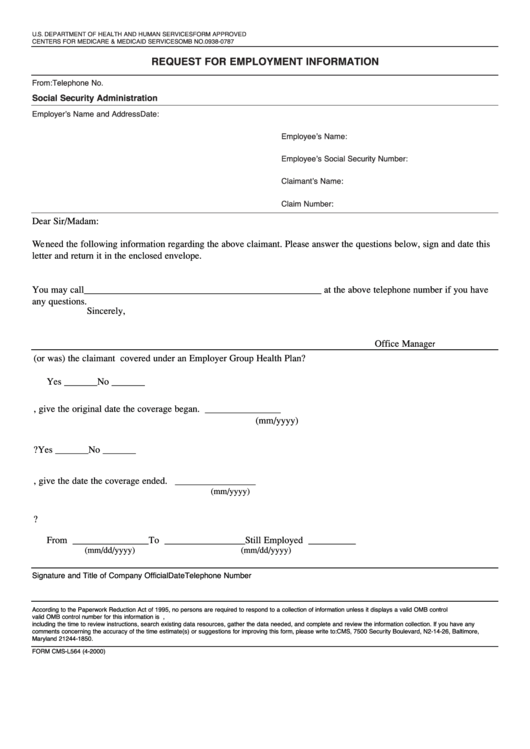
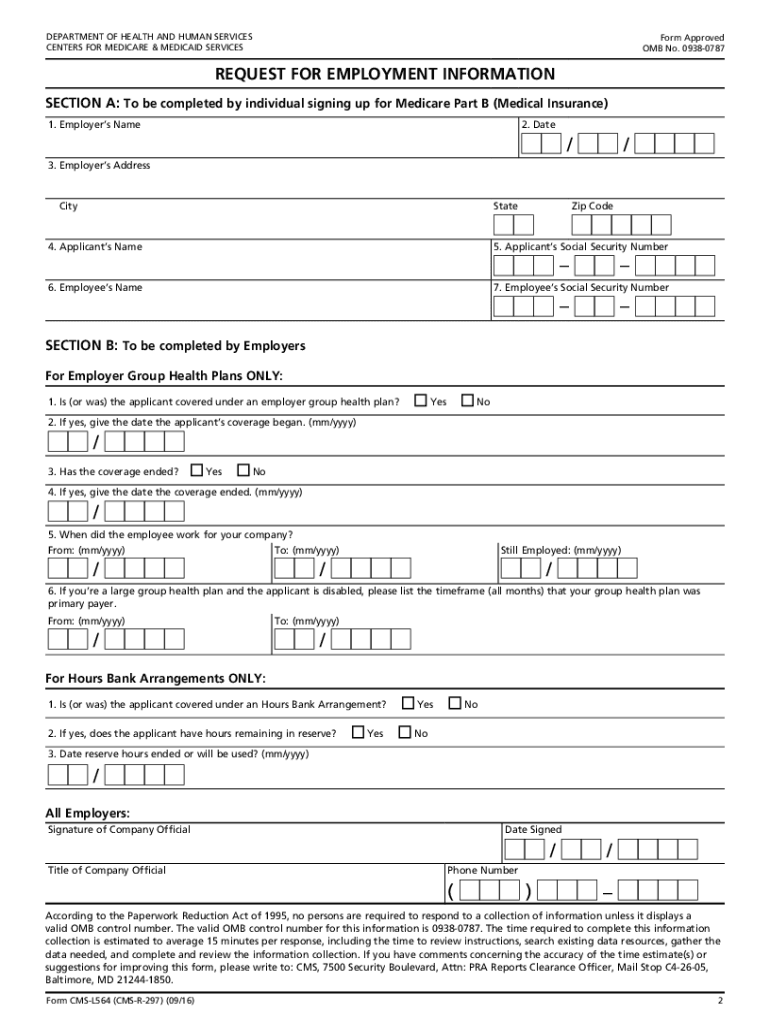
Web form approved omb no. Web find and fill out the correct form cms l564 printable. Write the name of your employer. Notice of denial of medical coverage/payment (integrated denial notice) Web cms l564 form printable. 06/2023departme nt of health and human services centers for medicare & medicaid servicesrequest for employment information cms 40b form i want part b coverage to begin. The person applying for medicare completes all of section a. Download your information to pdf before printing. You can also fax your enrollment forms and evidence of employment and health coverage to your local social security office. Department of health and human services centers for medicare & medicaid services form approved omb no. Write the date that you’re filling out the request for employment. Web this form is used for proof of group health care coverage based on current employment. Easily fill out pdf blank, edit, and sign them. Use the redaction tool to black out any sensitive information, such as social security numbers or personal addresses. Giving the social security administration proof you’re eligible to sign up for part b if: It is used only by those who have their plan covered by the entities where they work. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Open it up with online editor and begin altering. • your employer will need to complete the second half of the form with your employment dates and dates of your group health plan coverage. This document can be a lifesaver for those who skipped the gep and iep deadlines.
• Your Employer Will Need To Complete The Second Half Of The Form With Your Employment Dates And Dates Of Your Group Health Plan Coverage.
Concerned parties names, places of residence and phone numbers etc. What is the purpose of this form? The following provides access and/or information for many cms forms. If you have a special situation, fill out the application for medicare part a and b — special enrollment period (exceptional conditions.
Open It Up With Online Editor And Begin Altering.
This information is needed to process your medicare enrollment application. Web download and print to pdf. Their spouses can join the plan as well and fill this template out. Get everything done in minutes.
Notice Of Denial Of Medical Coverage/Payment (Integrated Denial Notice)
Get help with this form the employer that provides the group health plan coverage completes the information about your health care coverage and dates of employment. Web this form is used for proof of group health care coverage based on current employment. Web cms forms list. Use the redaction tool to black out any sensitive information, such as social security numbers or personal addresses.
Check Out How Easy It Is To Complete And Esign Documents Online Using Fillable Templates And A Powerful Editor.
According to the paperwork reduction act of 1995, no persons are required to respond to a collection of information unless it displays a valid omb control number. Department of health and human services centers for medicare & medicaid services form approved omb no. Giving the social security administration proof you’re eligible to sign up for part b if: Web find and fill out the correct form cms l564 printable.